
Our Analysis of Under-vaccination in India
- Mar 31
- 3 min read
Updated: Apr 1
Introduction
In late 2025, Suvita’s Data and Innovation Team looked into national and global datasets to better understand the remaining under-immunisation gap in India. More specifically, we sought to answer the question: Are there still sufficiently large and geographically concentrated groups of under-vaccinated children in India who remain reachable through targeted interventions? The answer to this question will inform our strategy over the coming years.
While the Indian government has launched several initiatives aimed at strengthening routine immunisation coverage(these include the introduction of the digital U-WIN platform, implementation of Intensified Mission Indradhanush 5.0 in 2023, and increasing policy attention toward identifying and reaching zero-dose children.), the most recent nationally representative survey providing district-level estimates of vaccination coverage in India, NFHS-5 conducted in 2019-21, is now several years old.
Our analysis primarily focused on Full Immunisation Coverage (FIC) as the key metric to understand under-vaccination. FIC measures the proportion of children who receive all basic routine vaccines in their first year of life. Using recent national estimates of vaccination coverage along with population projections, we estimated the number of children missing basic vaccines each year and examined how these children are distributed across states and districts in the country.
Key Findings
Despite overall progress, India still has a large absolute number of infants missing basic vaccines every year. This number has fallen from around 10 million children in 2015 to about 4 million children in 2025. Suvita’s recent global comparison using IHME 2024 Measles-1 estimates shows that India has the second-largest number of under-vaccinated children globally, exceeded only by Nigeria by a narrow margin.
Roughly half of under-vaccinated children are located in three states: Uttar Pradesh, Bihar, and Maharashtra. States with a large number of undervaccinated children also exhibit higher vaccine-preventable disease mortality burdens.

Figure 1: Countries with >0.5 Million Under-vaccinated Children for Measles 1
Our findings also show substantial heterogeneity among districts in the country. Around 15 percent of districts account for nearly half of the national number of under-immunised children. Bihar and Maharashtra, where Suvita operates, account for nearly a quarter of India’s under-vaccination numbers, with half of the states’ unmet need concentrated in just 18 districts (about 25 percent of districts within these states) that have both large absolute numbers (>10,000) of under-vaccinated children and coverage below 80 percent.
Many high-burden districts in India are large enough to rival entire low-income countries typically prioritised for global health interventions. Pune district within the state of Maharashtra, for example, had a population of 9.4 million in the 2011 Census – similar to Papua New Guinea or South Sudan at the time. A small number of high-burden districts in India can therefore match or exceed the under-vaccination needs of entire countries. As the figure below shows, targeting just 18 high-need districts across Bihar and Maharashtra – states where Suvita currently operates – would reach an estimated 0.41 million under-vaccinated children, exceeding the burden of several high-need countries individually and rivalling them collectively. Under-vaccination is also uneven within districts. Districts with low average coverage often contain pockets of substantially higher need alongside areas with relatively high coverage.
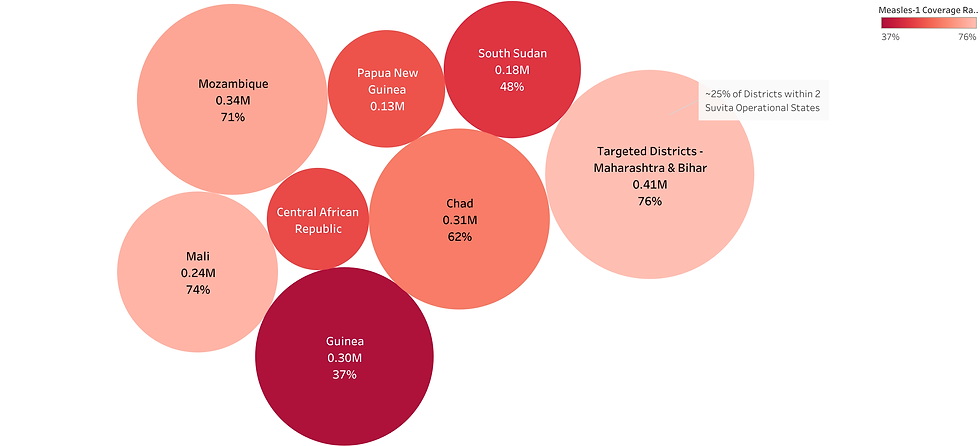
Figure 2: Comparison of under-vaccination burden in selected high-need districts of India and entire countries
We also found that the demand-side barriers continue to account for the majority of reported reasons for under-vaccination. Earlier evidence from 2009 suggested that around 76 percent of reasons for missed vaccination were demand-driven, majorly dominated by lack of perceived need and lack of knowledge of vaccination. More recent evidence (2024) suggests that demand-side barriers still account for roughly 65 percent of reasons, but their composition has shifted. Awareness gaps remain important, but fear of side effects is becoming increasingly prominent alongside refusal or hesitancy.
Patterns of under-vaccination are also associated with broader socioeconomic factors such as lower antenatal care coverage, lower maternal education levels, and lower household wealth.
Conclusions and Implications
Our analysis suggests that under-vaccination in India is a geographically concentrated challenge, rather than a uniformly distributed national problem. This implies that interventions focusing on high-need districts and specific sub-populations may be particularly effective in addressing the remaining gaps in immunisation coverage.
Because expanding into new geographies entails higher fixed operational costs than in areas where operations already exist, prioritisation should consider both the scale and severity of the problem and the implications for cost-effectiveness. In practice, this means prioritising districts that combine large absolute numbers of under-vaccinated children with substantial coverage gaps.
Because the majority of reported reasons for under-vaccination are demand-related, with increasing concerns about side effects and vaccine refusal, programme design should continue to adapt and iteratively test approaches that respond to changing behavioural and trust-related barriers in immunisation.
